Chronic illness care needs to be proactive, population-based, and centered around the needs of patients who are the ultimate managers of their illnesses.
Improving Chronic Illness Care
Developing a proactive model for population-based, patient-centered chronic illness care
The challenge
As people age and the burden of chronic illness grows, our health system needs to adapt. Instead of a system designed to provide reactive, acute care, chronic illness care needs to be proactive, population-based, and centered around the needs of patients who are the ultimate managers of their illnesses. Yet our funding systems still largely favor the old way of working. Primary care practices are strapped for time and entrenched hierarchies make team-based care rarer than it should be. Ultimately, people with chronic illnesses pay the price — with less than half of patients receiving recommended care.
These realities are felt even more acutely in Federally Qualified Health Centers, where the majority of patients live below 200% of the federal poverty level and face a variety of social risks. How then can we leverage what we know about how to provide high-quality, equitable chronic illness care to make change real in practices and with patients?
The work
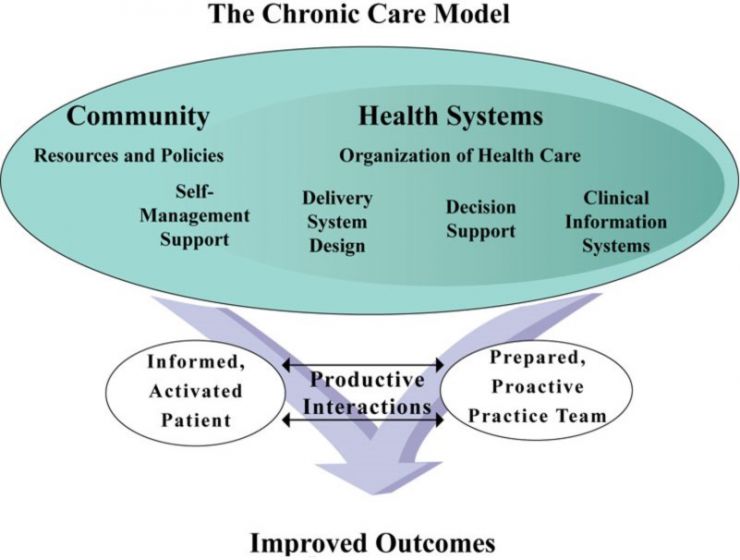
Understand evidence-based approaches to chronic illness care and draft the Chronic Care Model
Convene a national expert panel to finalize components and representation of the Chronic Care Model
Develop assessment tools for health systems (Assessment of Chronic Illness Care) and patients (Patient Assessment of Care for Chronic Conditions) to understand current state and change over time in implementing the Chronic Care Model
Develop and train health systems in the Chronic Care Model
Disburse substantial research funding to partners to explore the effectiveness of the Chronic Care Model and to further develop its components and implementation approaches
Partner with the Institute for Healthcare Improvement and the Bureau of Primary Health Care to launch National Health Disparities Collaboratives, involving more than 500 Federally Qualified Health Centers (2000 to 2006)
Establish a robust dissemination portal
What we learned
Busy primary care practices can make substantive changes in the domains of the Chronic Care Model, including clinical information systems, decision support, delivery system design, self-management, and community linkages.
In practices that implement the Chronic Care Model, patients receive better care and are more knowledgeable and empowered to care for their conditions.
Practices that implement more domains perform better on chronic illness care process and outcome measures than those that implement fewer.
After 1 year, most practices sustain changes and spread to new sites or conditions.
Most randomized controlled trials of the Chronic Care Model showed improvements in patient well-being across a wide range of chronic conditions.
Efforts to implement the Chronic Care Model work best when accompanied by a change package or specific set of activities, an evidence-based approach to guiding practices through the changes (e.g., learning collaboratives or practice coaching), and a quality improvement approach within the practice to create change (e.g., the Model for Improvement).
Despite what we know about the Chronic Care Model’s effectiveness, challenges to implementing and sustaining large-scale changes in chronic illness care persist. This is due to payment structures that do not support population health management, the need for new roles and training for care team members, and difficulty understanding and addressing social risks with community resources that are often poorly integrated with primary care.
Provided the framework for innovative programs that provide comprehensive care to people who live with chronic illness and other complex needs, such as the Vayu Health Diabetes Program
Extended and improved untold individual lives and health care practices
Featured publications
Coleman K, Austin BT, Brach C, Wagner EH. Evidence On The Chronic Care Model In The New Millennium. Health Aff (Millwood). 2009 Jan-Feb;28(1):75-85. doi: 10.1377/hlthaff.28.1.75. PubMed
Bodenheimer T, Wagner EH, Grumbach K. Improving Primary Care for Patients with Chronic Illness: The Chronic Care Model, Part 2. JAMA. 2002;288(15):1909–1914. doi: 10.1001/jama.288.15.1909. PubMed
Bodenheimer T, Wagner EH, Grumbach K. Improving Primary Care for Patients with Chronic Illness. JAMA. 2002 Oct 9;288(14):1775-9. doi: 10.1001/jama.288.14.1775. PubMed
Wagner EH, Austin BT, Davis C, Hindmarsh M, Schaefer J, Bonomi A. Improving Chronic Illness Care: Translating Evidence into Action. Health Aff (Millwood). Nov-Dec 2001;20(6):64-78. doi: 10.1377/hlthaff.20.6.64. PubMed
Wagner EH, Glasgow RE, Davis C, Bonomi AE, Provost L, McCulloch D, Carver P, Sixta C. Quality improvement in chronic illness care: a collaborative approach. Jt Comm J Qual Improv. 2001 Feb;27(2):63-80. doi: 10.1016/s1070-3241(01)27007-2. PubMed
Wagner EH. Chronic Disease Management: What Will It Take to Improve Care for Chronic Illness? Eff Clin Pract. Aug-Sep 1998;1(1):2-4. PubMed
Wagner EH, Austin BT, Von Korff M. Organizing Care for Patients with Chronic Illness. Milbank Quarterly. 1996;74(4):511–544. PubMed
PROJECT SNAPSHOT
FUNDER
Robert Wood Johnson Foundation
PARTNERS
Institute for Healthcare Advancement
Bureau of Primary Health Care
Primary care systems nationwide
KEY CAPABILITIES
Model development
Assessment development
Technical assistance
Learning collaboratives
Dissemination